
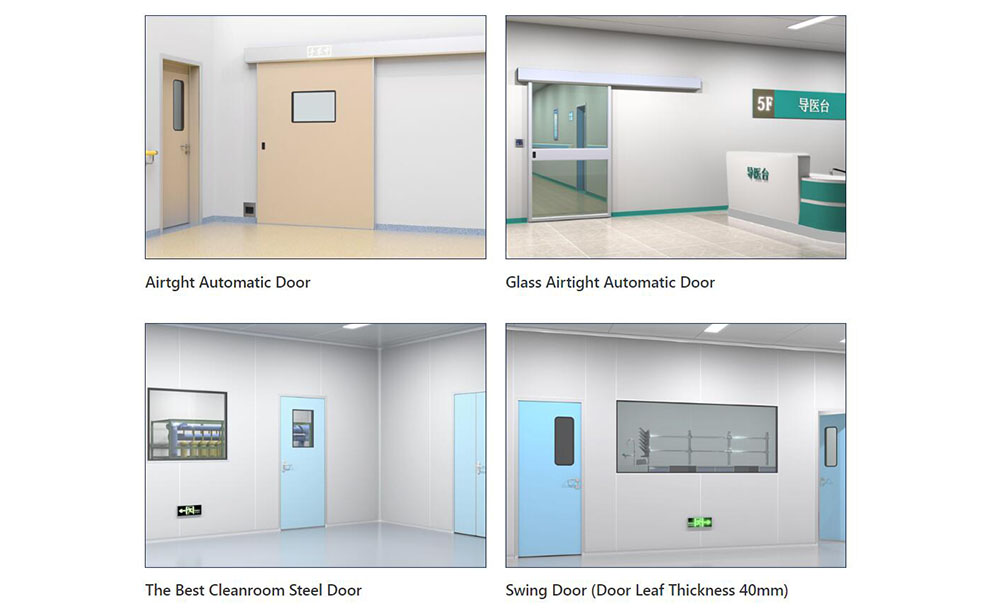
5 Hospital Door Mistakes That Cost Facilities $50K/Year

I. Executive Summary
Hospital doors are high-frequency clinical traffic nodes, not static building materials. In a typical 300-bed facility (800–1,200 doors), over 35% serve critical zones like ERs, ICUs, and ORs. Poor asset management and design lead to ~$50,000 in annual hidden OpEx losses—spanning HVAC overload, emergency repairs, compliance penalties, workflow inefficiency, and accelerated depreciation.
This article identifies five engineering-level mistakes behind these costs and outlines evidence-based solutions aligned with FGI, ASHRAE, ANSI/BHMA, and NFPA standards. By adopting TCO modeling, IoT-driven predictive maintenance, and traffic-optimized design, facilities can transition from reactive replacements to intelligent, cost-effective door operations.
II. Mistake 1: Prioritizing Upfront Cost Over Total Cost of Ownership
During renovations or routine replacements, many hospitals rely on unit purchase price as the primary decision metric, inadvertently introducing commercial-grade hollow metal doors into high-traffic clinical environments. However, healthcare operating conditions are exceptionally harsh: hundreds of daily cart and stretcher impacts, multiple daily cleanings with potent chlorine or quaternary ammonium disinfectants, and continuous exposure to humid air accelerate structural fatigue and surface coating degradation in standard doors. Industry field data shows that facilities not using professional healthcare doors experience hardware failure rates (hinges, closers, locks) up to 40% higher than standardized systems. Within 18 to 24 months, door surfaces develop micro-cracks and peeling, creating colonization sites for pathogens like MRSA and Aspergillus, directly leading to infection control audit deductions.
From an engineering economics perspective, true cost must be evaluated using a Total Cost of Ownership model. Saving $150–$200 per door by selecting light-duty systems inevitably leads to concentrated structural failures within 3 to 5 years. Emergency contractor replacements typically carry a premium of $300–$800 per unit, compounded by clinical corridor disruptions that delay bed turnover. Under straight-line depreciation, non-compliant doors have near-zero residual value, whereas medical-grade heavy-duty doors retain 15%–20% hardware replacement value in years 8–10.
Engineering Solutions:
- Specify ≥18-gauge cold-rolled steel with polyurethane or high-density mineral wool impact-resistant cores in bidding specifications.
- Strictly verify standard doorway width and frame tolerance to ensure clearance meets clinical transport requirements, avoiding post-installation cutting that compromises fire or airtight integrity.
- All primary egress routes must be equipped with a fire rated door meeting NFPA 80 and ASTM E119 standards (typically 60/90 minutes), integrated with heat-activated self-closing mechanisms and smoke-expansion seals.
- Require integrated supplier warranties (5-year structural, 3-year electro-mechanical) and include doors in the facility depreciation ledger. Conduct 10-year TCO retrospective audits to shift procurement from lowest bid to optimal Life Cycle Cost.
III. Mistake 2: Overlooking Hermetic Sealing & Pressure Differential Integrity
Airflow management in operating rooms, bone marrow transplant units, and negative pressure isolation rooms is an absolute red line for infection control. Yet, to control budgets, some projects install standard swing or sliding doors in these critical zones without dynamic sealing or pressure interlock systems. According to ASHRAE 170-2021, an operating room door must maintain positive pressure (+0.01 to +0.03 inches of water column), while negative pressure isolation rooms require -0.01 inches. When doors open or seals fail, the pressure gradient collapses instantly. The HVAC system compensates by consuming an additional 15%–22% energy, causing long-term chiller overload, shortened HEPA filter lifespan, and soaring energy costs. Critically, compromised airtightness directly elevates airborne pathogen transmission risks, violating CDC environmental infection control guidelines.
Engineering Solutions:
- Specify a hermetic door for high-grade clean and isolation zones. The door frame and leaf must use integrated welding or seamless splicing to eliminate gaps that harbor dust and microbes.
- Install a high-performance door seal (perimeter compression gaskets with automatic drop seals) to create a physical close-to-seal loop, keeping leakage rates strictly below 0.5 CFM/ft².
- For icu doors and similar critical areas, integrate high-precision micro-pressure differential sensors into the door structure. Signals should feed directly into the Building Management System to automatically trigger Variable Air Volume dampers during door cycles, maintaining pressure stability.
- Maintenance teams must conduct quarterly smoke pencil tests and archive airtightness compliance logs, ensuring strict alignment with GB 50333 and FGI airtightness mandates.
IV. Mistake 3: Ignoring ADA Compliance & Ergonomic Traffic Flow Design
Clinical traffic design directly impacts emergency response efficiency and patient safety. In reality, many older or poorly renovated corridors suffer from insufficient clear width, excessive manual opening force (>5 lbs), and lack of power assist. During emergency transports, ICU bed movements, or wheelchair navigation, these physical bottlenecks force staff into repetitive high-force pushing and pulling. Ergonomic studies show that excessive opening force, compounded over hundreds of daily cycles, adds 15–30 minutes of unnecessary physical strain per nurse per shift, significantly increasing the risk of rotator cuff injuries and musculoskeletal disorders, thereby driving up occupational health insurance claims. Furthermore, non-compliant doors that cause patient falls or equipment collisions expose facilities to ADA compliance fines ranging from $10,000 to $50,000 per violation, alongside civil litigation.
Engineering Solutions:
- Replace high-frequency clinical passage doors with ADA compliant hospital doors, strictly limiting opening force to ≤5 lbs (22N) and equipping push plates with low-mounted, accessible hardware.
- Egress and safety corridors must universally feature a push bar door mechanism paired with lever handles, ensuring single-handed, wheelchair-friendly operation in strict accordance with NFPA 101 Life Safety Code.
- Patient rooms and consultation spaces should utilize a door with window, featuring safety-rated glass and privacy tinting. This allows clinical staff to monitor patient vitals without physical entry, reducing unnecessary disruptions while enabling rapid visual communication when needed.
- Ensure a minimum 60”×60” clear floor space on the pull side to prevent swing encroachment into traffic flow. Integrate pedestrian heat mapping to dynamically optimize automatic door dwell times and sensor range, reducing idle cycles while maximizing throughput.
V. Mistake 4: Relying on Reactive Maintenance Instead of Predictive Monitoring
Traditional hospital facilities management often relies on quarterly inspections and break-fix reporting, leaving door systems without digital asset registries. When sensors fail, tracks accumulate debris, or motor brushes wear down, issues are typically discovered only after clinical disruptions occur, such as emergency department corridor jams or operating room door failures. This reactive model is costly: emergency contractor labor carries a 30%–50% premium, and critical part shortages cause 24–72 hours of downtime. Without digital oversight, facilities frequently neglect standardized execution of the hospital door maintenance checklist, allowing minor wear to escalate into major failures.
Engineering Solutions:
- Deploy Industrial IoT smart door controllers to continuously monitor cycle counts, motor current draw, rail vibration spectra, and seal wear indices. Process data at the edge and transmit via standard protocols to cloud or local servers.
- Integrate data streams into facility CMMS platforms. Machine learning algorithms establish equipment health baselines and auto-generate predictive work orders. For example, exceeding 150,000 cycles per year triggers deep lubrication and track alignment; periodic current spikes indicate impending bearing failure requiring preemptive replacement.
- In emergency and ICU zones, fully implement a touchless hospital door system using microwave radar, gesture recognition, or RFID credentialing. This eliminates physical contact, drastically reducing cross-contamination risks and mechanical wear.
- Maintain an N+1 critical spare parts inventory and enforce 4-hour SLA response contracts, compressing unplanned downtime to clinically tolerable thresholds.
VI. Mistake 5: Mismatching Door Operation Types to Clinical Workflow Zones
Many hospitals apply a one-size-fits-all door specification strategy, failing to zone based on sterility levels, urgency, and traffic profiles. For instance, using manual swing doors in emergency resuscitation bays impedes stretcher transit; installing light-duty automatic doors in logistics corridors leads to track deformation from frequent impacts; deploying heavy, noisy doors in general wards disrupts patient sleep cycles. This mismatch accelerates physical degradation, increases cross-contamination risks via dirty and clean path interference, and wastes clinical time. Lean healthcare calculations show that a 15-second delay per door cycle, across 1,000 daily passages, accumulates to roughly 4.1 hours of lost clinical productivity per facility daily, indirectly depressing bed turnover rates and performance scores.
Engineering Solutions: Implement a standardized Department-Door Configuration Matrix for precise matching and path segregation:
- Emergency / Labor & Delivery / ICU: Prioritize an automatic sliding door integrated with anti-pinch sensors and fail-safe breakaway release mechanisms to guarantee uninterrupted life-support access. Compliant sliding door installation must utilize heavy-duty rollers and dual anti-derailment safeguards, rated for ≥300 kg loads.
- General Wards / Clinics: Use swing doors with acoustic seals and low-energy hydraulic closers, balancing acoustic privacy with operational convenience.
- Laboratories / Clean Utility / Sterile Storage: Specify hygienic doors and cleanroom doors fabricated from 304/316L stainless steel or antibacterial high-pressure laminates. Surfaces must withstand caustic cleaning agents, and frame-to-wall junctions require full medical-grade silicone sealing to eradicate microbial harborage points. At the system level, integrate door control logic with nurse call systems and security access controls to enable emergency priority routing and tiered access management. Hardware should feature modular tracks and quick-install frames, enabling future workflow upgrades without clinical downtime.
VII. Conclusion & Strategic Next Steps
A hospital door is never an isolated component; it is a critical intersection of clinical safety, infection control, energy management, and asset operations. The $50,000 annual hidden loss is merely a conservative baseline. By elevating door strategy from point replacement to enterprise-level digital asset management, facilities will achieve compounding returns in compliance audit pass rates, clinical staff efficiency, ESG certification metrics, and patient experience scores. We recommend fully integrating door control systems into hospital BIM facility models, enabling data interoperability with HVAC, nurse call, and building automation to create a truly smart healthcare micro-circulation.
-
 Cleanroom Glass Windows Are The Key to Maintaining a Clean Environment
Cleanroom Glass Windows Are The Key to Maintaining a Clean Environment -
 Top Aluminium Profile Manufacturers in China: Leading the Global Market
Top Aluminium Profile Manufacturers in China: Leading the Global Market -
 The Evolution of Air Tight Sliding Doors
The Evolution of Air Tight Sliding Doors -
 AHU Aluminium Profile: A Comprehensive Guide
AHU Aluminium Profile: A Comprehensive Guide -
 The Importance of Choosing the Right Cleanroom Door in Vietnam
The Importance of Choosing the Right Cleanroom Door in Vietnam -
 The Benefits of Hospital Automatic Doors: Enhancing Efficiency and Safety
The Benefits of Hospital Automatic Doors: Enhancing Efficiency and Safety -
.jpg) The Best Bathroom Door Manufacturers - Unlocking Endless Possibilities!
The Best Bathroom Door Manufacturers - Unlocking Endless Possibilities! -
 Unlock the Possibilities with AJ Manufacturing Doors
Unlock the Possibilities with AJ Manufacturing Doors -
 Make a Statement with Manufactured Home Interior Doors!
Make a Statement with Manufactured Home Interior Doors! -
 what is aluminum profile? Aluminum Profiles for Your Home is the best option
what is aluminum profile? Aluminum Profiles for Your Home is the best option
-
 Cleanroom Sliding Door Selection Guide for GMP Facilities
Cleanroom Sliding Door Selection Guide for GMP Facilities -
 Hygienic Doors Selection Guide: Food, Pharma, Healthcare
Hygienic Doors Selection Guide: Food, Pharma, Healthcare -
 X-Ray Room Doors for Hospitals: Shielding, Access and Cleanability
X-Ray Room Doors for Hospitals: Shielding, Access and Cleanability -
Cleanroom Roll-Up Doors for Fast Access in Controlled Areas
-
 Medical Swing Doors vs Sliding Doors: How to Choose for Healthcare Spaces
Medical Swing Doors vs Sliding Doors: How to Choose for Healthcare Spaces -
 Cleanroom Vision Panel Doors: Visibility Without Compromising Hygiene
Cleanroom Vision Panel Doors: Visibility Without Compromising Hygiene -
 Fire Rated Cleanroom Doors for Controlled Environments
Fire Rated Cleanroom Doors for Controlled Environments -
 Cleanroom Double Doors for Equipment Access and Material Transfer
Cleanroom Double Doors for Equipment Access and Material Transfer -
 Laboratory Doors for Chemical, Biotech and Testing Facilities
Laboratory Doors for Chemical, Biotech and Testing Facilities -
 Pharmaceutical Facility Doors: Choosing the Right Door for Each Production Zone
Pharmaceutical Facility Doors: Choosing the Right Door for Each Production Zone





-

Home
-

Tel
-

Email
-

Contact

Guangzhou Yizhong Aluminum Industry Co., Ltd.
We are always providing our customers with reliable products and considerate services.
We are always providing our customers with reliable products and considerate services.
Speak Your Mind