
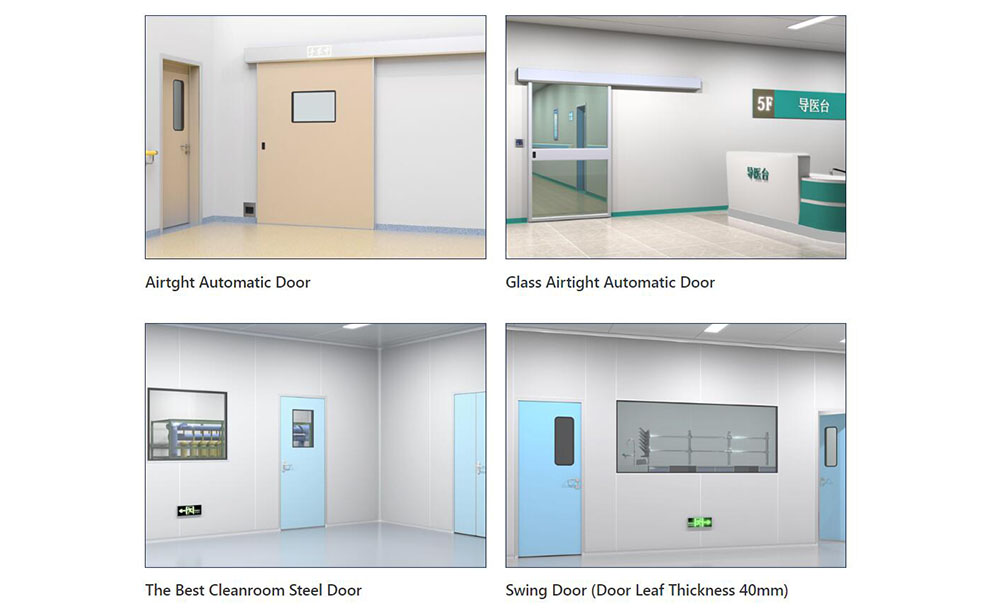
Medical Swing Doors vs Sliding Doors: How to Choose for Healthcare Spaces

1. Why Healthcare Door Selection Is a Systemic Engineering Decision
In modern healthcare facility management, hospital door system selection has evolved significantly beyond mere aesthetics or budget constraints. Consequently, it is now recognized as a critical engineering decision that directly impacts clinical workflow, infection control, regulatory compliance, and MEP coordination.
Therefore, when evaluating medical swing doors versus sliding doors, project managers and engineering contractors must prioritize clinical workflows and airflow dynamics over visual preferences. Moreover, in healthcare environments, doors function as the first line of defense for pressure differential maintenance, material segregation, fire egress, and emergency clearance.
Specifically, this guide focuses strictly on healthcare-specific applications, including patient wards, treatment rooms, surgical support zones, imaging departments, and primary corridors. Accordingly, it addresses spatial utilization, infection control grading, accessibility standards, electromechanical integration, and total cost of ownership (TCO) from a technical standpoint. For projects seeking the optimal swing vs sliding doors for healthcare solution, upfront scenario matching and BIM-integrated planning prove far more cost-effective and code-compliant than retroactive field modifications.
2. Core Dimensional Comparison: Technical Trade-offs in Clinical Environments
The technical evaluation of medical doors requires matching spatial physics with clinical operational demands. As a result, the following five dimensions form the core assessment matrix for medical swing doors versus sliding doors, directly influencing long-term performance and hospital door clearance requirements.

2.1 Spatial Utilization and Circulation Planning
Primarily, swing doors require a defined swing arc. For instance, standard 900 mm to 1200 mm leaves typically demand a clear floor radius of ≥1.2 m. However, in corridors ≤2.1 m wide or high-density ward layouts, swing doors frequently create circulation conflicts with gurneys and IV poles. In contrast, sliding doors utilize a wall-parallel translation path, thereby maximizing clear opening width to ≥95% of the rough opening. Consequently, this significantly reduces the horizontal footprint, making them the preferred hospital corridor traffic flow doors for narrow passageways and nursing islands.
2.2 Infection Control and Surface Cleanability
Furthermore, clinical environments impose strict microbial control standards for high-touch surfaces. Regarding infection control doors, swing door hinges, floor closer housings, and bottom sweeps readily become airflow dead zones that routine cleaning cannot reach. Additionally, bottom seals degrade under frequent use, which allows floor-borne contaminants to bypass the threshold. Conversely, sliding doors typically feature overhead concealed tracks or bottomless suspension designs, providing continuous, seamless door faces with zero cleaning blind spots. Moreover, they withstand daily wiping with 500–1000 mg/L chlorine-based disinfectants and quaternary ammonium compounds. Therefore, operators and control modules should carry a minimum IP54 rating to withstand wet environments and high-frequency sanitation protocols.
2.3 Accessibility and Regulatory Compliance
In terms of accessibility, ADA-compliant medical doors mandate an opening force ≤5 lbs (22.2 N). Although swing doors require low-energy closers or assistive operators to meet this threshold, they retain a natural advantage in emergency egress, since NFPA 101 prioritizes swing doors for primary evacuation routes. On the other hand, sliding doors rely on EN 16005 and UL 325-compliant safety logic, including photocells, anti-pinch torque sensors, and redundant braking systems. Crucially, during power loss, they must be equipped with mechanical override mechanisms, allowing personnel to manually slide the leaf in ≤3 seconds.
2.4 MEP Integration and Pressure Control
Similarly, regarding MEP integration, swing doors can be retrofitted with electromechanical closers and access control for basic automation. Nevertheless, pressure sealing typically depends on single or dual silicone gaskets, which are suitable for standard zones with ΔP ≤5 Pa. By comparison, sliding doors utilize integrated operator drives with multi-layer airtight and watertight seals, commonly EPDM or medical-grade silicone composites. Specifically, in negative pressure isolation room doors and surgical anterooms, sliding configurations stabilize pressure cascades at ±5 to ±15 Pa, thereby reducing HVAC load fluctuations and supporting long-term hospital door maintenance and compliance.
2.5 Total Cost of Ownership (TCO)
Financially, swing doors carry lower initial procurement and installation costs and require no structural reinforcement. However, in high-frequency zones exceeding 50,000 annual cycles, hinge, closer, and gasket replacement intervals compress to 12–18 months. Conversely, sliding doors entail higher CAPEX due to structural load verification and track embedment. Yet, they deliver superior OPEX when maintained correctly. For example, operators are typically rated for ≥100,000 cycles, with track cleaning scheduled at 6–12 month intervals. Ultimately, over a 5–10 year horizon, sliding doors demonstrate stronger TCO performance in primary circulation nodes.
3. Zoned Application Guide for Healthcare Facilities
This section outlines scenario-specific recommendations and parameter thresholds. Accordingly, it is designed for direct inclusion in design development packages and tender technical specifications.

3.1 General Wards, Isolation Rooms, and ICUs
Clinically, sliding doors are the preferred choice. Gurney ingress/egress and visitor traffic demand maximum clear opening width (≥1200 mm recommended), and sliding doors effectively eliminate swing arc conflicts with corridor traffic. Key Parameters: Antimicrobial surface treatments, vision panel coverage of 15–20%, and replaceable medical-grade bottom seals are required. Furthermore, isolation rooms and ICUs require enhanced airtightness to sustain negative pressure gradients. This aligns directly with the prevailing industry consensus for swing vs sliding doors for ICU environments. Reference: Hospital Room Door Options: Enhance Patient Care
3.2 Emergency Department and Trauma Bays
In high-acuity zones, automatic sliding doors are strongly recommended. These areas operate under high-cycle, rapid-response conditions. Key Parameters: Dual-track redundancy and anti-jamming drive logic are essential for continuous stretcher movement. Additionally, manual override response must occur within ≤3 seconds to ensure rescue workflows remain uninterrupted during power loss. Moreover, door assemblies must feature impact-resistant kick plates (≥1.2 mm 304 stainless steel) and fire alarm interlock release logic per NFPA 101.
3.3 Surgical Support Zones
Selection here is function-driven. Scrub rooms and sterile preparation areas typically utilize swing doors to maintain unidirectional airflow and minimize electromechanical complexity. Key Parameters: Soiled utility corridors favor sliding doors for rapid cart transit. Technically, priorities include +5 to +10 Pa positive pressure maintenance, heavy-duty kick plates, and coordinated routing with airlock chambers. Consequently, fire-rated doors for healthcare facilities in these zones must meet minimum 45-minute fire resistance ratings. Reference: Custom Hospital Doors Engineered for Cleanrooms & HVAC
3.4 Imaging and Specialized Treatment Rooms
Material and structural engineering dictate selection in these spaces. MRI suites require non-ferromagnetic sliding doors to prevent radiofrequency field interference. Key Parameters: Tracks and hardware must utilize aluminum-magnesium alloys or austenitic stainless steel. Meanwhile, CT and DR rooms can utilize standard sliding doors. Conversely, radiation shielding zones rely on heavy-duty composite swing doors, requiring hinge load verification (80–150 kg per leaf) to ensure RF shielding continuity and equipotential grounding.
3.5 Public Corridors and Nursing Station Hubs
Traffic density ultimately determines configuration. Low-volume corridors may specify swing doors to reduce initial investment. Key Parameters: High-traffic hubs or areas with BIM-identified congestion nodes should utilize sliding doors to decouple circulation paths. To validate this, engineering reviews should incorporate CFD airflow modeling and peak cart transit frequency (>80 movements/hour) to prevent swing arcs from becoming pedestrian bottlenecks.
4. Critical Technical Parameters for Detailed Design Verification
Once door selection enters the construction documentation phase, contractors and MEP teams must verify the following parameters upfront to prevent field rework. As such, this checklist establishes the baseline for hospital door installation best practices.
- Rough Opening Dimensions and Wall Construction: Light gauge steel partitions require overhead structural reinforcement. Specifically, overhead sliding door tracks typically demand a distributed load capacity of ≥1.5 kN/m. Conversely, concrete walls permit direct chemical anchor embedment, while heavy lead-lined doors necessitate independent structural framing.
- Automation Level and Power Failure Logic: Zones must be classified based on risk profiles. Therefore, critical areas require UPS backup to maintain 4–8 hours of operator functionality. Additionally, fire integration must follow fail-safe principles, automatically unlocking upon power loss or fire alarm activation.
- Sealing Performance and Pressure Ratings: Designs must align with GB 51039-2014, EN 16005, and local standards to define airtightness classes (Class 2 or 3). Furthermore, negative pressure zones must verify threshold leakage rates at ΔP=10 Pa. Meanwhile, gasket materials must resist medical-grade disinfectants and exhibit UV/ozone aging resistance.
- Hardware Durability and Surface Finishes: All hardware must pass ≥500,000 cycle endurance testing per EN 1935 or ANSI/BHMA A156.8. Consequently, surface treatments should utilize antimicrobial coatings or electrostatic powder finishes. In terms of protection, minimum IP ratings are IP44 (standard) / IP54 (wet zones), and impact plates must be flush-mounted.
- Fire, Access, and Security Integration: Access control release logic must achieve ≤0.5 second unlocking. Moreover, smoke detector interlocks require hardwired or Modbus/BACnet integration. Crucially, emergency egress routes mandate panic hardware, and CCTV sightlines must cover the full door width without obstruction.
5. Four-Step Decision Workflow for Rapid Door Type Matching
To ensure precision, follow this standardized workflow to improve design accuracy. This guarantees that medical swing doors vs sliding doors selection aligns precisely with project-specific constraints.
Step 1: Define Zone Classification. Map spaces according to infection control zoning principles: clean, semi-contaminated, contaminated, restricted, and unrestricted. Subsequently, establish baseline airflow direction and routing vectors. Step 2: Quantify Peak Traffic Loads. Document daily transit frequency for gurneys, supply carts, and staff. In addition, identify emergency response time thresholds (e.g., ER zones requiring ≤15 second clearance) and quantify circulation pressure points. Step 3: Verify MEP and Pressure Requirements. Coordinate closely with HVAC engineers to confirm pressure setpoints and supply/exhaust interlock sequences. Thereafter, validate that door sealing grades can sustain system stability without causing HVAC short-cycling. Step 4: Model TCO and Maintenance Cycles. Build a 5–10 year total cost of ownership model incorporating annual cycle counts, structural retrofit expenses, and motor warranty terms. Finally, high-frequency zones should prioritize sliding doors; whereas low-frequency areas may optimize with heavy-duty swing doors.
6. Conclusion and Project Technical Assessment
Ultimately, the selection of medical door types serves as hidden infrastructure for clinical workflow and infection control. Therefore, decisions must be made in advance during the design refinement stage to avoid later compliance risks and modification costs. In practice, the final configuration of medical swing doors vs. sliding doors should strictly conform to clinical working conditions, structural load-bearing capacity, and electromechanical linkage logic.
To move forward, please provide a description of your project area distribution along with a list of basic doorway dimensions (width × height × wall material/thickness). Based on current medical building codes and engineering collaboration experience, we will help you identify suitable door type configuration paths, structural verification points, and technical evaluation references.
-
 Cleanroom Glass Windows Are The Key to Maintaining a Clean Environment
Cleanroom Glass Windows Are The Key to Maintaining a Clean Environment -
 Top Aluminium Profile Manufacturers in China: Leading the Global Market
Top Aluminium Profile Manufacturers in China: Leading the Global Market -
 The Evolution of Air Tight Sliding Doors
The Evolution of Air Tight Sliding Doors -
 AHU Aluminium Profile: A Comprehensive Guide
AHU Aluminium Profile: A Comprehensive Guide -
 The Importance of Choosing the Right Cleanroom Door in Vietnam
The Importance of Choosing the Right Cleanroom Door in Vietnam -
 The Benefits of Hospital Automatic Doors: Enhancing Efficiency and Safety
The Benefits of Hospital Automatic Doors: Enhancing Efficiency and Safety -
.jpg) The Best Bathroom Door Manufacturers - Unlocking Endless Possibilities!
The Best Bathroom Door Manufacturers - Unlocking Endless Possibilities! -
 Unlock the Possibilities with AJ Manufacturing Doors
Unlock the Possibilities with AJ Manufacturing Doors -
 Make a Statement with Manufactured Home Interior Doors!
Make a Statement with Manufactured Home Interior Doors! -
 what is aluminum profile? Aluminum Profiles for Your Home is the best option
what is aluminum profile? Aluminum Profiles for Your Home is the best option
-
 Cleanroom Pass Doors: Getting Personnel and Material Flow Right
Cleanroom Pass Doors: Getting Personnel and Material Flow Right -
 What Is a Flush Cleanroom Door and Why Does It Matter
What Is a Flush Cleanroom Door and Why Does It Matter -
 Hermetic Door vs Airtight Door vs Hygienic Door: Key Differences
Hermetic Door vs Airtight Door vs Hygienic Door: Key Differences -
 Cleanroom Door Hardware: What Buyers Actually Get Wrong
Cleanroom Door Hardware: What Buyers Actually Get Wrong -
 How Do Cleanroom Doors Help Maintain Room Pressure
How Do Cleanroom Doors Help Maintain Room Pressure -
 Do Cleanroom Doors Need to Be Airtight
Do Cleanroom Doors Need to Be Airtight -
 Cleanroom Steel Door vs HPL Door: Which One Fits Your Project
Cleanroom Steel Door vs HPL Door: Which One Fits Your Project -
 Pharmaceutical Cleanroom Door Selection by Cleanroom Grade
Pharmaceutical Cleanroom Door Selection by Cleanroom Grade -
 USP Cleanroom Doors: What Should Buyers Check
USP Cleanroom Doors: What Should Buyers Check -
 What Are FDA-Compliant Cleanroom Doors?
What Are FDA-Compliant Cleanroom Doors?





-

Home
-

Tel
-

Email
-

Contact

Guangzhou Yizhong Aluminum Industry Co., Ltd.
We are always providing our customers with reliable products and considerate services.
We are always providing our customers with reliable products and considerate services.
Speak Your Mind