
ICU Doors: What Matters for Safety, Visibility and Infection Control
In critical care facility design, icu doors are far more than architectural partitions—they are essential clinical infrastructure. Operating continuously under heavy traffic, rigorous disinfection cycles, and strict pressure differentials, these assemblies directly impact patient safety, infection control, and emergency response. Generic procurement specifications often result in premature failure, cross-contamination risks, and workflow bottlenecks. This guide outlines the critical performance requirements for icu doors, providing actionable design parameters, compliance benchmarks, and procurement strategies aligned with modern hospital door specifications for healthcare planners, architects, and engineering buyers.
1. Observation Windows & Clinical Visibility: Balancing Monitoring and Privacy
Clinical monitoring in ICUs relies heavily on non-contact visualization. The observation window directly dictates staff response times to bedside emergencies. Window design must strictly adhere to ergonomic and optical performance benchmarks:
- Sightline Positioning: The window centerline should be set 1.25–1.45m above the floor, accommodating both standing rounds and seated monitoring sightlines. This reduces cervical strain from frequent bending and optimizes nursing station visibility.
- Optical Distortion Control: Must use low-reflectance (<5%) anti-fog laminated safety glass, with optical distortion controlled to ≤0.5%. This prevents refractive distortion from interfering with bedside monitor waveform readings or wide-angle camera fields of view.
- Privacy Switching Logic: Polymer Dispersed Liquid Crystal (PDLC) glass must clearly define its power-fail state. Clinical protocols typically require a Fail-Safe transparent state (remains clear on power loss) for emergency observation, or a UPS-backed Fail-Secure opaque state. Surface scratch-resistant coatings must be compatible with chlorine-based and hydrogen peroxide disinfectants.
- Digital Interface Provisioning: Window frames must pre-wire dry-contact terminals for BMS/nurse station integration, enabling status signal feedback and access control linkage. Post-installation core drilling must be avoided to preserve structural integrity and the air barrier.
Design Tip: Require third-party optical distortion test reports (per ASTM D1003) and PDLC power-fail sequence diagrams during submittal. Verify protocol compatibility with the facility’s central management system (BACnet/Modbus RTU). FGI Guidelines 2022 explicitly recommends that ICU observation windows eliminate optical blind spots; early-stage sightline simulation with nursing leadership is advised.
2. Infection Control & Hygienic Design: Zero-Compromise Cleanroom Construction

The ICU is the core zone for multidrug-resistant organism (MDRO) and airborne pathogen containment. Door assembly construction must adhere to seamless, chemical-resistant, and low-VOC principles. Key requirements for infection control doors include:
- Surface Flatness & Recessed Hardware: Door leaf surface flatness tolerance must be ≤1.0mm. Exposed fasteners, panel joints, or decorative grooves are prohibited. Hinges, crash plates, and door closers must be fully recessed or housed in medical-grade dust shields to eliminate microbial colonization niches.
- Chemical Resistance Validation: Antimicrobial coatings must align with actual facility disinfection SOPs. Final acceptance requires documented evidence of ≥5,000 cycles of high-level disinfection (HLD/IDL)擦拭 testing without chalking, cracking, or discoloration (per ASTM D1308/D2248), ensuring verified HLD chemical resistance.
- Indoor Air Quality Control: Surface VOC emissions must comply with GREENGUARD Gold or LEED v4 EQc2 standards, with TVOC ≤0.5 mg/m³. This prevents off-gassing from exacerbating respiratory load in mechanically ventilated patients.
- Perimeter Sealing & Pressure Management: Negative/positive pressure ICU door air leakage must be controlled to ≤0.5 m³/(h·m). Gaskets should use medical-grade EPDM or platinum-cured silicone, with compression set <15%. Paired with ±1Pa micro-differential pressure sensors, the system enables dynamic compensation to prevent pressure decay. Medical grade door frames must be seamlessly integrated with wall assemblies to eliminate dust-trapping gaps.
Engineering Practice Insight: During an ICU renovation at a top-tier tertiary hospital in East China, the initial specification omitted HLD chemical resistance thresholds. After 18 months of operation, the door leaf finish developed micro-fissures from repeated chemical exposure, increasing fomite retention risk. Replacement with ASTM D1308-validated seamless antimicrobial panels eliminated the issue. Specifications must clearly distinguish between antimicrobial efficacy and chemical durability. Procurement teams should verify ozone and UV aging test data (ASTM D2240/D412) for perimeter seals to guarantee <15% compression set over a 5-year lifecycle.
3. Traffic Efficiency & Workflow Optimization: Redundancy for Emergency Scenarios

ICU workflows are characterized by high frequency, heavy loads, and emergency urgency. The actuation logic and clear opening of icu doors directly determine the usability of the golden rescue window. Traffic and automation system configurations must meet the following standards:
- Clear Width & Swing Arc: Minimum effective clear opening ≥1.20m (1.35m recommended) to accommodate ventilator carts, stretchers, infusion pump arrays, and dual-staff escorting simultaneously. Swing doors must be equipped with 180° heavy-duty wall/floor stops and hydraulic buffer closers (EN 1154 Grade 4–6).
- Touchless Activation & Anti-Pinch Protection: high-frequency automatic sliding doors should utilize 24GHz millimeter-wave radar paired with dual-technology infrared sensors, covering a 0.3–1.5m detection zone. Anti-pinch force thresholds must be strictly ≤150N (per EN 16005). Opening speed is adjustable between 0.3–0.5 m/s, with hold-open time programmable in 3–10s increments to match varying clinical rhythms.
- Power-Fail Emergency & Access Tiering: critical care environment doors must operate on a Fail-Safe (power-off open) logic to prioritize fire egress and emergency access. UPS backup must provide ≥30 minutes of runtime, and ADA-compliant mechanical manual override devices are mandatory.
- Workflow Physical Segregation: Visitor zones and clinical clean zones must be hard-separated via access control permissions, aligned with ICU visitation policies to minimize unnecessary cross-traffic and aerosol dispersion. fail-safe door hardware must include mandatory manual override functionality.
Engineering Implementation Tip: Automatic door drive systems must specify a motor MTBF ≥50,000 cycles. Procurement should require hardwired integration test reports with the facility’s Fire Alarm System (FAS), ensuring electromagnetic locks disengage and free-passage mode activates within 0.5 seconds of a fire alarm signal. During commissioning, simulate fully loaded cart transit to validate radar blind-spot coverage and deceleration curves, preventing peak-hour transit bottlenecks.
4. Acoustic Performance & Noise Control: The Hidden Variable Affecting Clinical Outcomes

WHO and FGI guidelines mandate that ICU nighttime ambient noise remain ≤35–40 dB(A). As a critical acoustic weak point in the building envelope, door performance directly impacts patient delirium rates and staff cognitive load. Acoustic intervention and clinical outcomes should align with the following metrics:
- STC Rating & Core Construction: icu doors assemblies must achieve a STC rating for hospital doors of ≥38 (standard patient rooms typically range 28–32). Solid damping composite cores paired with dual-perimeter sealing significantly attenuate 500–2000Hz high-frequency noise.
- Perimeter Acoustic Sealing: Automatic drop seals can provide an additional 10–15dB of sound attenuation when engaged. Silent door closers must maintain a terminal impact sound pressure level ≤55dB(A) to prevent transient impact noise from triggering false monitor alarms or disturbing light-sleeping patients.
- Clinical Intervention Value: Evidence-based data indicates that deploying acoustic hospital doors with STC 40+ ratings, combined with acoustic ceiling clouds and resilient flooring, yields the following clinical benefits:
- 12–18% reduction in ICU delirium incidence
- 22% improvement in nighttime staff communication clarity
- ~15% decrease in handoff information omission rates
- BIM Coordination Requirements: Acoustic design must be integrated during early medical planning phases. Routing MEP penetrations through door frames post-installation must be strictly prohibited to preserve acoustic breaks. airborne infection isolation room doors require additional focus on coupling negative-pressure sealing with acoustic attenuation.
Design Tip: Require full-frequency sound transmission loss curves (per ASTM E90 or ISO 10140) rather than relying solely on a single STC value. Note: Laboratory STC ratings must be verified post-construction via field sound transmission class testing (ASTM E336). Proper installation using elastomeric sealants and floating frame assemblies is critical to eliminating rigid sound bridges.
5. Safety, Compliance & Lifecycle Reliability
Stringent healthcare building codes impose rigid requirements on the fire resistance, impact durability, and emergency logic of icu doors. Safety validation and healthcare door compliance checklists must cover the following core items:
- Fire & Smoke Certification: Fire resistance rating ≥1.0h (per GB 50016-2014(2018)/NFPA 80/NFPA 101-2024), equipped with heat-expanding fire seals and CCC/UL-listed composite fire-rated glazing. Frame-to-wall connections must utilize Class A firestop materials.
- Impact Resistance & Structural Integrity: The lower 300mm of the door leaf (bed-end impact zone) must feature reinforced steel framing paired with impact-resistant HPL or 304 stainless steel cladding. Must pass ASTM E695 heavy-pendulum impact testing (≥50J energy absorption), with surface scratch resistance meeting EN 438-2 HGS grade.
- Safety Logic Tiering: Egress corridors/negative-pressure isolation doors must operate on Fail-Safe logic; pharmacy/secure equipment rooms must use Fail-Secure (power-off locked). All automatic doors must include mechanical manual override devices compliant with ANSI A117.1 accessibility standards.
- Ingress Protection (IP) Ratings: Drive motors and controllers should carry a minimum IP54 rating to prevent cleaning disinfectant mist from infiltrating control boards. BIM medical door families must contain complete fire-rating, hardware, and electrical interface parameters to facilitate MEP clash detection.
Compliance Tip: Submittal packages must include third-party fire test reports, structural impact certifications, and power-fail transition sequence diagrams. Avoid conflating baseline fire certification with medical-grade high-cycle durability. NFPA 101-2024 Life Safety Code explicitly prohibits mechanical obstructions in critical care egress paths; procurement teams must verify hinge load ratings against door closer torque curves.
6. Engineering Procurement & Selection Guide: From Parameter Compliance to TCO Decision-Making
Procurement must move beyond lowest-bid traps and establish a Total Cost of Ownership (TCO) evaluation model. TCO hospital door procurement decision frameworks should strictly adhere to the following structure:
Technical Submittal Checklist
- Third-party fire, acoustic, air-leakage, and antimicrobial test reports (CMA/CNAS accredited)
- Medical door BIM families (LOD 300), 1:1 installation detail drawings, hardware compatibility matrices
- Warranties tiered by component: Door leaf assembly ≥10 years / Drive system ≥3 years / Wear items ≥2 years
Lifecycle Cost Accounting Dimensions
- Initial procurement cost typically represents only 30–40% of total project expenditure
- Factor in detailing labor, HLD-induced finish replacement cycles, and MTTR (Mean Time To Repair)
- High-reliability systems may carry 15–20% higher CAPEX but can reduce OPEX by over 35%
Vendor Screening Core Metrics
- Proven delivery track record for tertiary hospital ICUs and infection control commissioning experience
- Open protocol support (BACnet IP / dry-contact / Modbus RTU)
- 24/7 emergency response SLA and regional critical spare parts inventory
- Provision of door assembly pressure-flow (P-Q) performance curves to verify dynamic HVAC compatibility
Bidding & Evaluation Model
- Adopt a weighted scoring system: Technical 70% / Commercial 30%
- Treat verified STC values, air leakage rates, MTBF, and chemical resistance cycles as disqualifying thresholds
- Tie contract payment milestones to joint infection control commissioning sign-off and 72-hour continuous fault-free operation testing
Procurement Implementation Tip: Include "approved manufacturer lists for critical components" and "interchangeability requirements for replacement parts" in tender documents. Avoid vendor lock-in that inflates long-term maintenance costs. For large-scale greenfield hospital projects, require bidders to submit a 5-year operational data dashboard for equivalent icu doors installations as a technical scoring differentiator.
Conclusion: Defining the Systemic Value of icu doors Through Clinical Process Design
ICU doors are not the endpoint of architectural finishes, but the starting point of clinical workflow systems. Visibility, infection control, traffic efficiency, acoustic intervention, and safety compliance are deeply interdependent. Compromising any single dimension will be exponentially magnified under clinical high-cycle usage. Facility planners and design teams must integrate icu doors into early-stage medical workflow simulations and MEP BIM coordination from day one. Procurement teams must anchor decisions to TCO and lifecycle reliability. Only by elevating doors from basic building materials to clinical support equipment, and strictly adhering to hospital door specifications and infection control doors engineering standards, can healthcare organizations truly construct critical care environments that are safe, efficient, and aligned with evidence-based medicine.
-
 Cleanroom Glass Windows Are The Key to Maintaining a Clean Environment
Cleanroom Glass Windows Are The Key to Maintaining a Clean Environment -
 Top Aluminium Profile Manufacturers in China: Leading the Global Market
Top Aluminium Profile Manufacturers in China: Leading the Global Market -
 The Evolution of Air Tight Sliding Doors
The Evolution of Air Tight Sliding Doors -
 AHU Aluminium Profile: A Comprehensive Guide
AHU Aluminium Profile: A Comprehensive Guide -
 The Importance of Choosing the Right Cleanroom Door in Vietnam
The Importance of Choosing the Right Cleanroom Door in Vietnam -
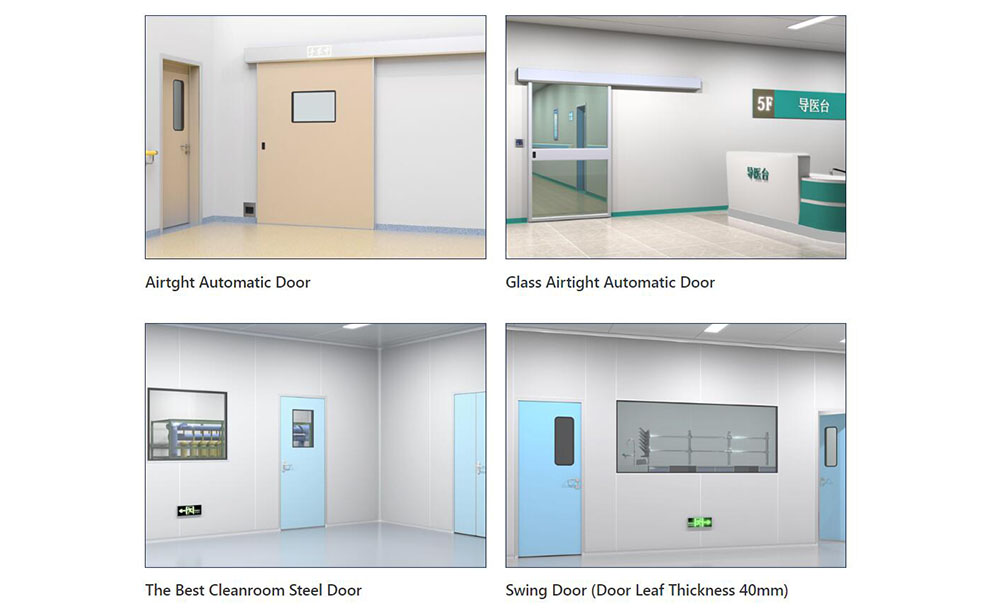
 The Benefits of Hospital Automatic Doors: Enhancing Efficiency and Safety
The Benefits of Hospital Automatic Doors: Enhancing Efficiency and Safety -
.jpg) The Best Bathroom Door Manufacturers - Unlocking Endless Possibilities!
The Best Bathroom Door Manufacturers - Unlocking Endless Possibilities! -
 Unlock the Possibilities with AJ Manufacturing Doors
Unlock the Possibilities with AJ Manufacturing Doors -
 Make a Statement with Manufactured Home Interior Doors!
Make a Statement with Manufactured Home Interior Doors! -
 what is aluminum profile? Aluminum Profiles for Your Home is the best option
what is aluminum profile? Aluminum Profiles for Your Home is the best option
-
 Cleanroom Sliding Door Selection Guide for GMP Facilities
Cleanroom Sliding Door Selection Guide for GMP Facilities -
 Hygienic Doors Selection Guide: Food, Pharma, Healthcare
Hygienic Doors Selection Guide: Food, Pharma, Healthcare -
 X-Ray Room Doors for Hospitals: Shielding, Access and Cleanability
X-Ray Room Doors for Hospitals: Shielding, Access and Cleanability -
Cleanroom Roll-Up Doors for Fast Access in Controlled Areas
-
 Medical Swing Doors vs Sliding Doors: How to Choose for Healthcare Spaces
Medical Swing Doors vs Sliding Doors: How to Choose for Healthcare Spaces -
 Cleanroom Vision Panel Doors: Visibility Without Compromising Hygiene
Cleanroom Vision Panel Doors: Visibility Without Compromising Hygiene -
 Fire Rated Cleanroom Doors for Controlled Environments
Fire Rated Cleanroom Doors for Controlled Environments -
 Cleanroom Double Doors for Equipment Access and Material Transfer
Cleanroom Double Doors for Equipment Access and Material Transfer -
 Laboratory Doors for Chemical, Biotech and Testing Facilities
Laboratory Doors for Chemical, Biotech and Testing Facilities -
 Pharmaceutical Facility Doors: Choosing the Right Door for Each Production Zone
Pharmaceutical Facility Doors: Choosing the Right Door for Each Production Zone





-

Home
-

Tel
-

Email
-

Contact

Guangzhou Yizhong Aluminum Industry Co., Ltd.
We are always providing our customers with reliable products and considerate services.
We are always providing our customers with reliable products and considerate services.
Speak Your Mind